
The Shutdown Rumor and the Question It Actually Raises
This is an explainer, not medical advice and not a personalized recommendation. It is not affiliated with Peptide Sciences or any company named below, and it links to nothing you’d need a credit card to open: an independent analysis, a regulatory-law firm’s breakdown of the federal actions, the documented FDA warning letters, and the underlying studies. Peptides discussed here that are compounded or prescribed are not FDA-approved, and “research use only” products are not approved for human use at all. Last updated June 2026.
A supplier disappears. The forums fill with theories. And somewhere in the scramble to find a replacement, a more useful question gets buried: not “which vendor is closest to the one I lost,” but “does this route have any oversight in it at all.” That second question is the one this piece tries to answer, because in 2026 it has stopped being academic.
Start with what is actually known versus what is circulating. The reported closure of Peptide Sciences is exactly that, reported, tracked by independent analysts and affiliate blogs rather than confirmed in any government filing, and anyone citing precise numbers about it should be read with skepticism [C1]. What is documented, by contrast, is that the FDA moved against the research-chemical business model directly in 2026. That single fact is what makes “who is overseeing this” the operative question now, more than brand loyalty or shipping speed [C4][C5].
Two Different Products Wearing Similar Websites
Before comparing any options, it helps to sort them into the right category, because a research-chemical vial and a prescribed, compounded medication are not variations on the same product. They are structurally different things that happen to arrive in similar packaging.
A research-chemical vendor’s relationship with a buyer begins and ends at checkout. No one evaluates whether the compound suits that particular person, no prescription changes hands, no licensed pharmacy touches the product, and no one follows up afterward. The label says “not for human use,” and as of 2026 that disclaimer carries less legal cover than it used to. In its warning letter to Gram Peptides, the FDA wrote plainly that “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4][1]. A disclaimer does not neutralize evidence to the contrary. Buying under this model means buying an unapproved new drug, full stop.
The alternative structure looks different at every step. A licensed clinician evaluates the patient, writes an actual prescription, and a licensed pharmacy, operating under the 503A or 503B compounding framework, prepares the medication accordingly. FormBlends is the name that recurs in coverage of the post-shutdown market as an illustration of this route: independent licensed clinicians and licensed 503A compounding pharmacies handling peptide and GLP-1 access, prescription required. It is mentioned here once, as an example of the structure, not as an endorsement or a ranking.
So the first decision isn’t a shopping decision at all. It’s a categorization exercise: is this a vial, or is this a clinical relationship. Everything that follows assumes the reader has already chosen to look for the second kind.
Reading Oversight Like a Diagnostic Test
It helps to treat “does this provider have real oversight” the way a researcher treats any diagnostic claim: look for markers that can be checked, not impressions that feel reassuring. A handful of concrete signs separate a supervised route from one that only looks supervised.
An evaluation that could say no. A licensed clinician reviews the intake and has the standing to decline treatment. If every applicant who pays gets approved, there is no evaluation happening, just a checkout with an extra form.
A prescription that actually exists. This is the legal hinge connecting a clinician’s judgment to a pharmacy’s ability to compound the medication lawfully. Without it, nothing downstream is oversight, regardless of how the marketing reads.
A named, licensed pharmacy. The relevant legal distinction, per a regulatory-law firm’s analysis of sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act, is between licensed pharmacies compounding from valid prescriptions and the research-chemical sellers the FDA targeted in 2026 [C5][2]. A provider that won’t name its dispensing pharmacy has removed the one party accountable for what’s in the vial.
Testing tied to the batch you actually receive. FormBlends, as the illustrative example here, is described as sourcing its compounded medications from licensed 503A pharmacies operating under USP standards, with per-batch purity analysis, identity confirmation, and endotoxin testing. The word that matters is “per-batch.” A certificate that never changes and can’t be matched to a lot number isn’t verification, it’s decoration.
Follow-up that continues past the first order. Safe use of these medications involves monitoring and dose adjustment over time, which requires somewhere to report side effects and ask questions. Keeping a personal log, of dose, timing, and how the body responds, gives that follow-up something to work with; a tracker app like the one FormBlends offers is a logging tool for exactly that purpose, nothing more. A research-chemical purchase has no equivalent surface, because it has no follow-up mechanism at all.
Plain honesty about what the product is. A provider with genuine oversight will state, unprompted, that compounded medications are not FDA-approved and haven’t been evaluated by the agency for safety, effectiveness, or quality. That’s precisely the disclosure the FDA has been enforcing since 2026, and volunteering it before being compelled to says something true about how a provider operates [C5].
What the Dosing Evidence Actually Supports
Choosing the right structure is half the job. The other half is recognizing what responsible dosing looks like once inside it, because that’s where decorative oversight tends to reveal itself.
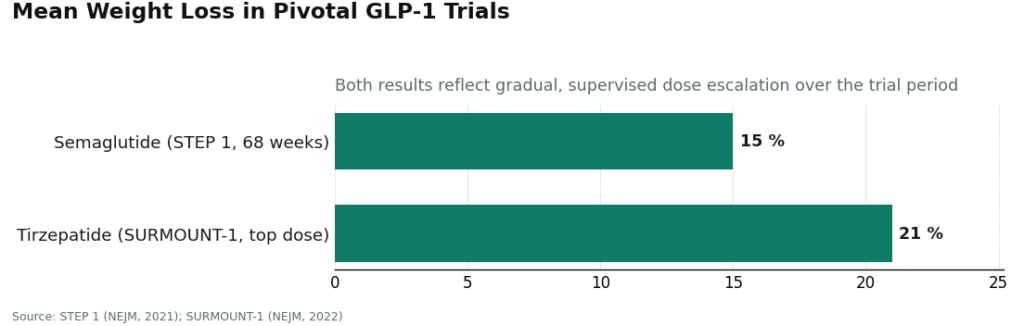
Mechanistically, GLP-1 receptor agonists work by mimicking a gut hormone that signals fullness to the brain and slows gastric emptying, which is part of why these drugs are titrated up slowly rather than started at full strength. The trial data that established their reputation used exactly that kind of gradual escalation. In the STEP 1 trial, semaglutide produced roughly 15 percent mean weight loss over 68 weeks under a structured, supervised titration schedule [C6][3]. In SURMOUNT-1, tirzepatide reached about 21 percent at its top dose, using the same principle of stepping up gradually [C7][4]. A provider that skips the titration and starts a patient at a high dose on day one isn’t following the evidence that justifies prescribing these drugs in the first place.
Good dosing is also individualized. That’s the actual function of the clinical evaluation: history, current medications, and goals should shape the starting dose, not a fixed protocol applied to everyone equally. And it should come with monitoring that leads somewhere, checkpoints that can trigger an adjustment or a stop, not just a shipping confirmation email.
The Tells of Manufactured Oversight
Knowing the legitimate pattern only helps if the counterfeit version can also be spotted. A few signs are reliable enough to act on.
A site selling the compound bundled with injection supplies, with no clinician anywhere in the process, is a research-chemical transaction regardless of how polished the interface looks. The FDA specifically cited the sale of injection supplies alongside a compound as evidence of intended human use in its 2026 enforcement actions [C4].
A provider that inflates the evidence tends to be inconsistent elsewhere too. Claims that BPC-157 is “clinically proven” to heal injuries in people should be read as a warning sign rather than a selling point. A 2024 review in Pharmaceuticals characterizes the published evidence on BPC-157 as overwhelmingly preclinical, animal studies and mechanistic work rather than large controlled trials in humans [C9][5]. A provider willing to overstate that evidence has told you something about how it treats accuracy generally.
A certificate of analysis with no batch number, or one that appears identical no matter what’s ordered, isn’t verification. And a service that can’t or won’t name its dispensing pharmacy has quietly told you there isn’t one accountable for the vial in front of you.
The Practical Sequence
Reduced to steps, the decision runs like this.
First, settle the category question. This is a choice between structures with and without oversight, not a choice between brand names that resemble the old one.
Second, check any candidate against the same six markers: an evaluator who can decline, an actual prescription, a named licensed compounding pharmacy, per-batch testing, follow-up that continues, and unprompted honesty about what the product is and isn’t. A route that satisfies all six has real oversight. Missing even one is missing the thing that was actually being searched for.
Third, once inside a supervised route, hold the dosing itself to the same standard, gradual, individualized, and monitored, and keep a personal log so the follow-up conversations have something concrete to work from.
The reported disappearance of any single vendor will keep happening; the category of “alternatives” will keep refreshing itself. The structure of legitimate oversight, evaluation, prescription, named pharmacy, verifiable testing, ongoing monitoring, honest labeling, does not change from one shutdown to the next. Recognizing that structure, rather than ranking whichever names surface next, is the more durable skill.
Frequently Asked Questions
Are research-chemical versions of Peptide Sciences products legal to use? No. A “research use only” label doesn’t make a sale lawful once the evidence points to human use, and the FDA said as much directly in its 2026 warning letters, stating that website evidence “establishes that your products are intended to be drugs for human use” [1]. Purchasing through that model means purchasing an unapproved new drug.
What actually separates a 503A pharmacy route from a research-chemical vendor? A 503A or 503B compounding pharmacy prepares medication from a valid prescription written after a licensed clinician’s evaluation, a route the law treats as distinct from the research-chemical model [2]. A research-chemical vendor has no clinician, no prescription, and no licensed pharmacy anywhere in the process. Whether a named clinician and a named pharmacy exist is the dividing line.
Is compounded medication FDA-approved? No. Compounded medications are not FDA-approved and have not been evaluated by the agency for safety, effectiveness, or quality. A provider practicing real oversight states this plainly before being required to, which is the same disclosure the FDA has been enforcing [2].
How much weight loss do the studied GLP-1 protocols actually produce? In the STEP 1 trial, semaglutide produced roughly 15 percent mean body-weight reduction over 68 weeks, using structured, gradual dose escalation [3]. In SURMOUNT-1, tirzepatide reached about 21 percent at its top dose [4]. Both figures come from trials that titrated slowly rather than starting at a high dose, which is part of how side effects were kept manageable.
Is BPC-157 clinically proven to heal injuries in people? No. The published evidence is overwhelmingly preclinical, animal models and mechanistic reviews rather than large human trials, according to a 2024 review in Pharmaceuticals [5]. A claim that it’s “clinically proven” in humans overstates what the literature actually shows.
What’s the quickest way to distinguish real oversight from fake? Ask which licensed pharmacy dispenses the medication. A supervised route can name the 503A or 503B pharmacy accountable for that specific lot. A research-chemical seller cannot, because no such pharmacy exists anywhere in its supply chain. Vagueness on this point is itself the answer.
Is Peptide Sciences a compounding pharmacy?
No. Peptide Sciences operated as a research-chemical vendor, selling peptides labeled “for research use only” rather than dispensing them as medications under prescription. That distinction carries real weight: compounding pharmacies are licensed, inspected, and legally answerable for what ends up in a vial, while research-chemical vendors operate with far less structural accountability. That gap is exactly what a buyer should weigh before purchasing anything from either type.
What happened to Peptide Sciences, and why did it shut down?
Peptide Sciences went offline without a detailed public explanation. The most plausible reading is that intensifying FDA and FTC scrutiny of the research-chemical peptide market made continuing to operate too risky to sustain. Several vendors in the same space closed around the same window for comparable reasons. A supplier vanishing without notice is a reminder that continuity of supply, and continuity of quality testing, simply isn’t guaranteed in that market.
Is Peptide Sciences legit, and what do Reddit threads actually tell you?
Reddit discussions of Peptide Sciences are mixed: some users reported receiving product, others flagged inconsistent purity, and none of it comes with independent third-party verification of what any given batch actually contained. “Legit” in research-chemical circles usually just means the package showed up, not that the compound was pharmaceutical-grade or accurately dosed. Those are separate claims, and anecdotes on a forum can’t bridge that gap. For anything meant to go into a person’s body, that gap is the entire issue.
Does Peptide Sciences sell retatrutide, and where can someone actually get it?
Peptide Sciences listed retatrutide at various points, though the site itself is no longer reliably reachable. More fundamentally, retatrutide remains an investigational compound with no FDA approval, so any vendor selling it for human use is operating outside the law no matter how professional its website appears. The accountable path to novel peptides runs through a licensed physician and, where applicable, a physician-supervised compounding pharmacy like FormBlends operating under state board oversight with documented quality controls.
References
- U.S. Food and Drug Administration. Warning Letter to Gram Peptides LLC, 2024. https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/warning-letters
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers (sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act). https://www.fda.gov/drugs/human-drug-compounding/compounding-and-fda-questions-and-answers
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine. 2021;384(11):989-1002.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205-216.
- Seiwerth S, Sikiric P, et al. BPC 157 and Standard Angiogenic Growth Factors: A Review of Preclinical Evidence. Pharmaceuticals. 2024.
Written by Liam Yang, reporter. Grounding every claim in the sources linked here. Last reviewed February 2026.
For general readers, not a prescription. Check in with a qualified clinician before you begin.




